
Lipoprotein(a): Key Insights for Clinical Practice
2022 ESC/EAS Consensus Statement Summary
Structure and Epidemiology
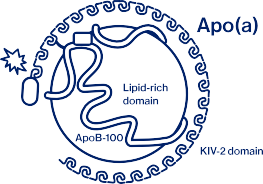
Lipoprotein(a) [Lp(a)] consists of an LDL particle with apolipoprotein(a) covalently bound to apoB100. Unlike other lipoproteins, Lp(a) levels are >90% genetically determined by the LPA locus, resulting in stable lifelong concentrations with low response to lifestyle modifications. Significant ethnic variation exists, with median levels approximately three times higher in Black (39 mg/dL) versus White populations (12 mg/dL). Approximately 20% of the global population has elevated levels, making Lp(a) one of the most common inherited cardio-vascular risk factors.

Cardiovascular Risk Assessment
Human genetic studies demonstrate Lp(a) as a causal risk factor linked to atherosclerotic cardiovascular disease, aortic valve stenosis, myocardial infarction, ischemic stroke (particularly in those < 60 years), and heart failure. The relation between Lp(a) concentration and these outcomes is continuous; elevated Lp(a) is a risk factor even at low LDL-C concentration. This risk remains significant also in patients with well-controlled LDL-C, highlighting Lp(a) as an independent residual risk factor. Notably, while Lp(a) increases arterial thrombotic risk, it is not considered a risk factor for venous thromboembolism.

Testing in Clinical Practice
The consensus recommends measuring Lp(a) once in all adults, ideally with the first lipid profile. Screening is also recommended in youth with a history of ischaemic stroke or a family history of premature ASCVD or high Lp(a) and no other identifiable risk factors. Cascade testing for high Lp(a) is recommended in the settings of familial hypercholesterolemia (FH), family history of (very) high Lp(a), and personal or family history of ASCVD.
Clinically relevant thresholds include:
- <30 mg/dL (<75 nmol/L): Lower risk
- 30-50 mg/dL (75-125 nmol/L): Intermediate risk
- >50 mg/dL (>125 nmol/L): Higher risk
Management Strategies
When elevated Lp(a) is detected, incorporate this finding into comprehensive cardiovascular risk assessment. The identification of elevated Lp(a) may necessitate reclassification to a higher cardiovascular risk category, warranting more intensive preventive strategies. Consider more aggressive LDL-C targets and optimization of other modifiable risk factors. In the absence of specific Lp(a)-lowering therapies, current management focuses on optimizing modifiable risk factors to mitigate the increased risk conferred by elevated Lp(a).

This summary highlights practical clinical implications from the 2022 European Society of Cardiology/European Atherosclerosis Society Consensus Statement on
Lipoprotein(a) in Atherosclerotic Cardiovascular Disease and Aortic Stenosis, European Heart Journal (2022) 43, 3925–3946.