
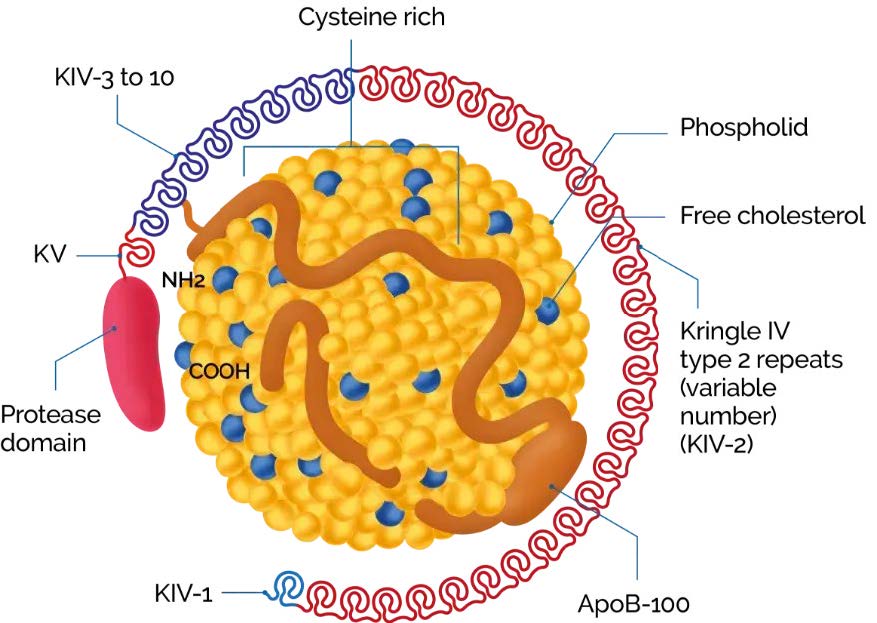
The structure of Lp(a)1
Lp(a) is an LDL-like particle, with a single apolipoprotein B100 (apoB), covalently linked by a disulphide bond to a single apolipoprotein(a) (apo(a)). The molecular mass of apo(a) can vary between 275 and 800 kDa due to the inheritance of>40 different allelic LPA variants encoding different numbers of kringle IV type 2 repeat sequences in this polypeptide. The rate of apo(a) synthesis and secretion is inversely related to its molecular mass, and consequently, individuals who produce the lower molecular mass apo(a) isoforms have higher serum Lp(a) levels than those who produce the higher molecular mass isoforms.1
KV, Kringle 5; KIV-1, Kringle 4 type 1; KIV-3 to 10, Kringle 4 types 3 to 10; ApoB-100, Apolipoprotein B100; NH2, NH2-terminal; COOH, C-terminus.
Adapted from Cegla J et al, 2019
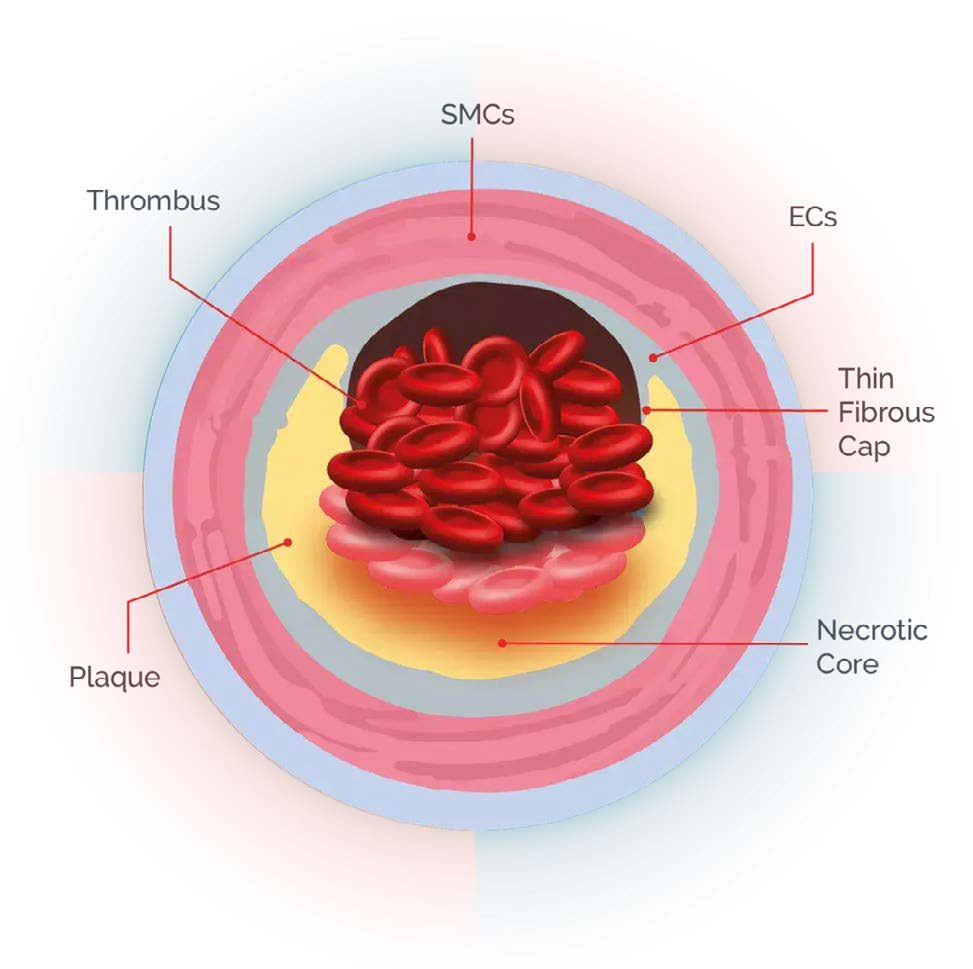
In patients with advanced stable coronary artery disease (CAD), elevated Lp(a) was associated with accelerated progression of the necrotic core.1 Patients with elevated Lp(a) may exhibit a more severe disease presentation, which refers to the complex atherosclerotic lesions that are more difficult to treat.2 In patients with acute coronary syndrome (ACS), elevated Lp(a) drives a higher prevalence of vulnerable plaque characteristics, including thin-cap fibroatheroma.3 Elevated Lp(a) levels are independently associated with plaque progression and vulnerable plaque characteristics.4,5
ACS, acute coronary syndrome; CAD, coronary artery disease; ECs, endothelial cells; FH, familial hypercholesterolemia; Lp(a), lipoprotein(a); SMCs, smooth muscle cells.
References: 1. Kaiser Y, et al. J Am Coll Cardiol. 2022;79(3):223–233. 2. Leistner D & Laguna-Fernandez A, et al. Eur J Prevent Cardiol. 2024;31(7):856-865. 3. Kato A, et al. Int J Cardiol Heart Vasc. 2022;43:101120. 4. Verweij SL, et al. J Clin Lipidol. 2018;12(3):597–603.e1 5. Garg PK, et al. J Cardiovasc Comput Tomogr. 2021;15(2):154–160.
Elevated Lp(a) may drive fast-progressing and vulnerable atherosclerotic plaques1-5